PMOS: Understanding the New Name for PCOS and What It Means for Women’s Health
May 14, 2026 02:25 PM
For decades, the condition commonly known as polycystic ovary syndrome (PCOS) has been one of the most misunderstood and underrecognized disorders affecting women’s health. In May 2026, an international global consensus formally adopted a new name: Polyendocrine Metabolic Ovarian Syndrome (PMOS). This landmark change, published in The Lancet, reflects a growing understanding that the condition extends far beyond the ovaries and impacts multiple hormonal and metabolic systems throughout the body.
The renaming emerged from a large international collaboration involving 56 academic, clinical, and patient advocacy organizations, along with input from more than 14,000 patients and healthcare professionals worldwide. The goal was not simply cosmetic rebranding, but rather a shift toward more accurate recognition of the condition’s true complexity and lifelong health implications.
Why the Name Changed
The term “polycystic ovary syndrome” has long been criticized for being both misleading and incomplete.
One major issue is that women with the condition do not actually develop ovarian cysts in the traditional medical sense. Instead, ultrasound findings typically show an increased number of immature ovarian follicles, sometimes referred to as excess antral follicles. Calling these “cysts” has created confusion for patients and even some healthcare providers.
The previous name also focused narrowly on the ovaries, despite the fact that the condition commonly involves:
- Insulin resistance
- Hormonal dysregulation
- Metabolic dysfunction
- Inflammation
- Cardiovascular risk factors
- Dermatologic manifestations
- Mood and psychological symptoms
As a result, many individuals experienced delayed diagnosis, fragmented care, and stigma surrounding fertility and body image. The new terminology aims to better represent the multisystem nature of the condition and encourage a more comprehensive approach to assessment and treatment.
What “PMOS” Means
Polyendocrine
The word polyendocrine reflects the involvement of multiple hormonal systems.
PMOS commonly affects:
- Ovarian hormone production
- Insulin signaling
- Adrenal androgen production
- Hypothalamic-pituitary regulation
Many patients experience elevated androgens such as testosterone, irregular ovulation, insulin resistance, and altered stress hormone patterns. This endocrine complexity helps explain why symptoms can vary so dramatically from person to person.
Metabolic
The inclusion of metabolic highlights one of the most clinically significant aspects of the condition.
Many individuals with PMOS experience:
- Insulin resistance
- Dyslipidemia
- Impaired glucose tolerance
- Increased abdominal adiposity
- Elevated cardiovascular risk
- Increased risk of type 2 diabetes
Importantly, metabolic dysfunction can occur even in individuals with normal body weight, emphasizing that PMOS is not simply a “weight-related” disorder.
Ovarian
The term ovarian remains because ovarian dysfunction is still central to the syndrome.
Common ovarian features include:
- Irregular ovulation
- Absent ovulation
- Follicular excess
- Menstrual irregularity
- Fertility challenges
Retaining “ovarian” acknowledges the reproductive implications while removing the inaccurate implication of cyst formation.
Syndrome
The word syndrome remains appropriate because PMOS is highly heterogeneous. No two patients present exactly the same way, and symptoms can evolve throughout the lifespan.
What Has NOT Changed
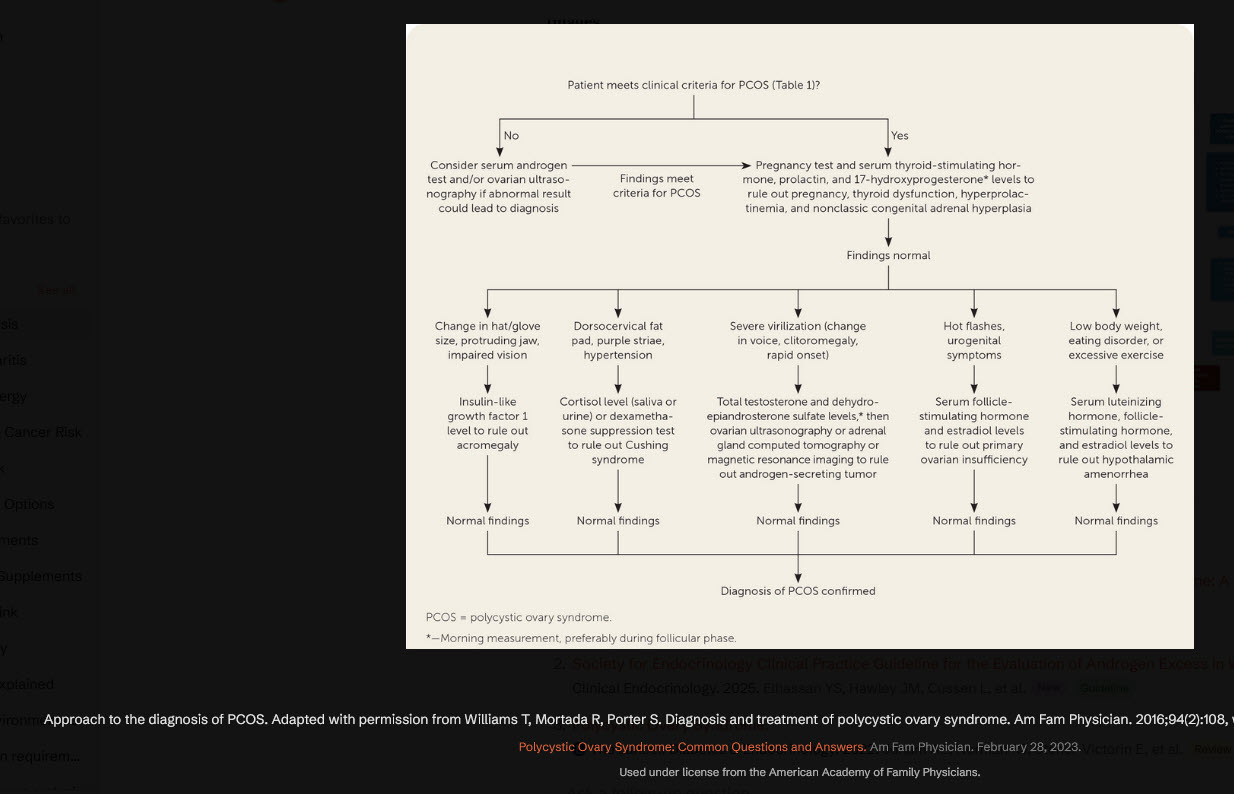
Despite the new terminology, the diagnostic criteria remain unchanged.
Diagnosis still requires two of the following three features:
- Clinical and/or biochemical hyperandrogenism
- Ovulatory dysfunction or irregular menstrual cycles
- Polycystic ovarian morphology on ultrasound or elevated anti-Müllerian hormone (AMH)
Similarly, current evidence-based treatment recommendations remain the same as those outlined in the 2023 international guidelines.
A More Holistic Clinical Perspective
Although treatment algorithms have not changed, the new framing may influence how clinicians approach patient care.
Earlier Metabolic Screening
The emphasis on metabolism reinforces the importance of routinely assessing:
- Blood glucose regulation
- Insulin resistance
- Lipid profiles
- Blood pressure
- Cardiovascular risk markers
Historically, some patients were evaluated primarily for fertility concerns while metabolic risks went underrecognized for years.
Lifelong Multisystem Care
PMOS is increasingly recognized as a lifelong condition that may affect:
- Reproductive health
- Mental health
- Cardiovascular health
- Sleep quality
- Skin and hair health
- Energy regulation
This broader perspective encourages more collaborative and integrative care models involving endocrinology, nutrition, mental health, sleep medicine, dermatology, and lifestyle medicine.
Weight-Neutral Care
Modern guidelines increasingly emphasize compassionate, weight-neutral approaches.
While weight loss may improve outcomes for some individuals, health optimization should not be reduced to a number on a scale. Lifestyle interventions—including nutrition, movement, sleep optimization, stress management, and metabolic support—can improve symptoms across a wide range of body sizes.
Emerging Areas of Research
The reconceptualization of PMOS as a metabolic-endocrine condition may accelerate research into newer therapeutic approaches.
Areas of growing interest include:
- GLP-1 receptor agonists
- Insulin-sensitizing therapies
- Incretin-based treatments
- Osteocalcin research
- Gut microbiome modulation
- Inflammation-targeted interventions
Researchers are also exploring how sleep, circadian rhythm disruption, environmental toxins, and chronic stress may influence disease progression and symptom severity.
Reducing Stigma and Diagnostic Delay
One of the most meaningful goals of the name change is reducing stigma and improving patient understanding.
Many individuals with PCOS previously reported confusion when told they had “cysts” despite never having ovarian cyst disease. Others felt their symptoms were minimized or fragmented across different specialties.
By reframing the condition as a systemic endocrine-metabolic disorder, PMOS may help:
- Improve earlier recognition
- Encourage broader screening
- Validate patient experiences
- Support interdisciplinary care
- Increase public awareness and research funding
Looking Ahead
The transition from PCOS to PMOS represents more than a terminology update. It reflects a major evolution in how the medical community understands one of the most common endocrine disorders affecting women worldwide.
Importantly, the new name does not change the lived experience of patients overnight, nor does it immediately alter treatment protocols. However, it does provide a more accurate and comprehensive framework—one that better captures the hormonal, metabolic, reproductive, and psychological dimensions of the condition.
As awareness grows, the shift to PMOS may ultimately improve diagnosis, reduce stigma, encourage earlier intervention, and foster more holistic patient-centered care.
References:
1.
Polyendocrine Metabolic Ovarian Syndrome, the New Name for Polycystic Ovary Syndrome: A Multistep Global Consensus Process.
Lancet. 2026. Teede HJ, Khomami MB, Morman R, et al.NewReview
2.
Society for Endocrinology Clinical Practice Guideline for the Evaluation of Androgen Excess in Women.
Clinical Endocrinology. 2025. Elhassan YS, Hawley JM, Cussen L, et al.NewGuideline
3.
Polycystic Ovary Syndrome.
The Lancet. Diabetes & Endocrinology. 2022. Joham AE, Norman RJ, Stener-Victorin E, et al.Review
4.
Polycystic Ovarian Morphology and Chronic Morbidity and Mortality in PCOS.
JAMA Network Open. 2025. Kugelman N, Morris DV, Bastrash MP, et al.NewObservational
5.
Recommendations From the 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome.
The Journal of Clinical Endocrinology and Metabolism. 2023. Teede HJ, Tay CT, Laven JJE, et al.